The prescription
opioid crisis of overdosing and overprescribing has reached
epic proportions, according to the North American media. Just last week, we learned that
91% of patients who survive opioid overdose are prescribed more opioids! The
CDC calls it
an epidemic, and notes there's been “a 200% increase in the rate of overdose deaths involving opioid pain relievers and heroin.” A recent paper in the
Annual Review of Public Health labels it a “public health crisis” and proposes
“interventions to address the epidemic of opioid addiction” (
Kolodny et al., 2015).
In the midst of this public and professional outcry, why on earth would anyone recommend opioid drugs as a treatment for severe depression and suicidal ideation??
Let's revisit the questions posed in my
previous post:
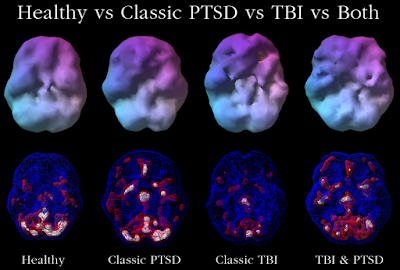
- Does the pain of mental anguish rely on the same neural machinery as physical pain?
- Can we treat these dreaded ailments with the same medications?
The opioid-for-depression proponents would answer both of those questions in the affirmative,
1 with some qualifications. First off, the actual medication in question (and its dose) is different from the typically abused
opiate /
opioid drug. As far as I can tell, no one is clamoring for narcotic analgesics like
OxyContin and
Vicodin to be used as antidepressants.
In his
2008 paper on the Psychotherapeutic Benefits of Opioid Agonist Therapy,
Dr. Peter L. Tenore reviewred the history of the Opium Cure and declared,
“Opioids have been used for centuries to treat a variety of psychiatric conditions with much success.” However, these drugs can be highly addictive (obviously) so he issued this caveat at the end of the paper:
It should be noted that opioids do not have FDA approval for the treatment of psychiatric disorders. The intent of this paper was not to suggest that practitioners should prescribe opioids in a manner not approved by the FDA, but rather it was to explore the mechanisms and develop hypotheses that might explain the observation that opioid-dependent psychiatric patients in appropriately certified opioid replacement therapy programs (i.e., methadone treatment programs) stabilize on higher opioid dosages than those without psychiatric diagnoses.
Methadone and especially low-dose
buprenorphine are the drugs being tested for their antidepressant efficacy, even in those who have no opioid abuse issues. Buprenorphine is a mixed partial μ/κ agonist with
complex actions, including:
- Antagonist (blocker) of κ-opioid receptors (KORs) that bind dynorphins (endogenous opioids associated with anxiety and dysphoria)
- Partial agonist at μ-opioid receptors (MORs), producing analgesic effects but with less euphoria and less respiratory depression than full agonists
Basic research in rodents suggests that KORs may be a promising target for potential psychiatric treatments in humans, based on improvements shown in standard behavioral assays such as the forced swim test and the elevated maze test (
Crowley & Kash, 2015).
2But there's still a long way to go. In addition to the difficulty of modeling mental anguish in animals, the complexity of the dynorphin/KOR system
— which can exhibit paradoxical and “convoluted” effects on behavior
3— presents a barrier to clinical translation.
In contrast, a very different approach uses affect modeling in an effort to accelerate drug development in neuropsychiatry (
Panksepp & Yovell, 2014). In this view, current models of depression have hindered new breakthroughs because of their focus on animal behaviors, instead of animal emotions. Panksepp maintains that separation distress and infant versions of
psychic pain,
excessive sadness, and
grief are mediated by the
PANIC system, which is
soothed by opioids. Chicks, kittens, puppies, and other infant animals emit
distress vocalizations when separated from their mothers. Rat pups emit ultrasonic vocalizations and
baby monkeys“coo”. These innate, reflexive, and
adaptive behaviors are reduced with low doses of morphine.
4Panksepp and colleagues have inferred that very strong and human-like emotions are associated with distress vocalizations.
![]()
By way of example, here is my adult cat. He's very affectionate and
chatty. He requires a lot of attention and doesn't like to be alone. Does he meow and miss me when I'm on vacation? I imagine he does. Do I think he feels psychic pain and grief while I'm gone? No.
Watt and Panskepp (2009) argue that depression is an evolutionarily conserved mechanism to terminate separation distress, drawing on psychoanalytic concepts like
object relations theory as well as the literature on neuropeptides and neuromodulators implicated in major depression.
Nopan Treatment of Acute SuicidalityThe research on separation distress in animals helped motivate a
clinical trial that was recently published in the
American Journal of Psychiatry (
Yovell et al., 2015). The initial daily dose of Nopan (0.1 or 0.2 mg sublingual buprenorphine hydrochloride) was relatively low, reaching a maximum dose of 0.8 mg daily by the end of the four week trial (mean = 0.44 mg). By way of comparison, the
maintenance dose for opioid dependence is 4 to 24 mg/day.
5 Analgesic effects are obtained at 0.1– 8 mg (according to
Heit, 2010), although Yovell et al. said their doses were subanalgesic.
Eighty-eight severely suicidal patients were enrolled in the double-blind, placebo-controlled trial, about 2/3 of whom had made at least one suicide attempt. Over half met criteria for
borderline personality disorder (BPD), which includes symptoms like affective instability, self-harm, high rates of substance abuse, and fear of abandonment (i.e., heightened separation distress). Although 50 patients had BPD, the other 48 did
not. If separation distress is a major motivating construct for the trial, it seems problematic to have a heterogeneous population on that dimension. Nevertheless...
Almost all were clinically unstable, and their ability to cooperate with the study team was compromised, as reflected in a high dropout rate (29.5%) during the first week of treatment.
This sort of study is very difficult to conduct, so it's not surprising that the completion rate was low (57%):
33 patients on buprenorphine, 17 on placebo (the original randomization was deliberately 2:1).
- click on image for a larger view -
Modified from Fig. S2 (Yovell et al., 2015). A portion of the flow diagram (starting from those who were enrolled).Importantly, participants with a lifetime history of opioid abuse were excluded. Buprenorphine is a
Schedule III controlled substance in the US (same as
ketamine), with a lower potential for abuse than heroin (Schedule I) and morphine, methadone, OxyContin, etc. (Schedule II).
6As we know, individuals with BPD have
high rates of
substance abuse. In
one study, 44% of patients seeking buprenorphine treatment for opioid addiction were diagnosed with BPD. Therefore, the investigators had to screen the participants very closely, in partnership with their regular clinical providers. Other exclusionary criteria were schizophrenia, current psychosis, and
ECT within the past month. Finally, there could be no substance or alcohol abuse or benzodiazepine dependence within the past 2 years.
Regarding patient demographics, 70% were female, 43% had major depression, 25% were currently hospitalized, 49% had experienced major stressors in the last year (but separation during past month in only 24%), 70% on antidepressants, 49% on
benzos, and about 20% on mood stabilizers and antipsychotics.
A week’s supply of medication (<5.6 mg, usually <2.8 mg) was not considered to present a high risk for suicide by overdose. Outpatients received the study medication for the following week during their weekly visits, and took it independently at home.
Another difficulty is that opioids have notable side effects, and this was true with the “ultra-low-dose” used here (
Yovell et al., 2015)
— which isn't really all that low.
One or more adverse events were reported in 77.2% of participants in the buprenorphine group and 54.8% of those in the placebo group (p=0.03). Among participants in the buprenorphine group, there were more reports of fatigue (49.1% compared with 22.6% in the placebo group), nausea (36.8% compared with 12.9%), dry mouth (29.8% compared with 9.7%), and constipation (26.3% compared with 9.7%).
The primary outcome measure was change in suicidal ideation after four weeks of treatment. To make up for high dropout, the Last Observation Carried Forward (LOCF) was used. In this way, data from all participants who received at least one dose of drug and one suicidal ideation score were included. However, LOCF is a flawed procedure that can overestimate effect sizes.
7The buprenorphine group had lower suicidal ideation than the placebo group at weeks 2 and 4, but an analysis restricted to patients who completed the study was not reported. Furthermore, the suicidal ideation scores were highly variable, and improvements in many secondary outcome measures (e.g., depression severity) didn't reach statistical significance (Fig. S3 below).
The authors acknowledged seven critical limitations, summarized below (the most egregious in
red):
- Outcome measures based on self-report. Clinician ratings of suicidality, depression, and overall functioning should be part of any future trial.
- Participants were unstable and severely suicidal; many had BPD; high dropout rates. Are the findings applicable to more stable, less severely suicidal patients?
- Flexible and gradual dosing limits inferences about the optimal dosage of buprenorphine to treat suicidal ideation.
- Heterogeneity of the study population [e.g., why were both BPD and non-BPD included?] and its modest size limited ability to stratify results by dose, gender, and diagnosis.
- Study did not assess nonsuicidal self-injury, which is associated with BPD, mental pain, and abnormalities in the endogenous opioid system.
- I'll add that a case series on buprenorphine for NSSI was not cited.
Trial did not include an extended follow-up period to allow assessment of possible long-term effects, including the possibility of developing drug craving or rebound suicidality. Despite its favorable safety profile, buprenorphine is potentially addictive and possibly lethal. The authors end by stating the “results do not support the widespread, long-term, or nonexperimental use of buprenorphine for suicidality.” In other words, don't open buprenorphine clinics to treat severe depression and suicidal ideation! [
ketamine infusion clinics, I'm looking at you].
People suffering from suicidal thoughts and actions deserve the best possible care, yet many researchers and clinicians shy away from conducting clinical trials.
Ketamine seems to be the exception, where 24 studies are listed in
ClinicalTrials.gov. While the present study has a long list of admitted flaws that make me wonder why it was published in
AJP, the authors are in the admirable position of trying to help an extremely vulnerable population.
Read Part 1, Social Pain Revisited: Opioids for Severe Suicidal Ideation.Footnotes1 But not surprisingly, many others don't agree with this strategy
— e.g., Opioids in Depression: Not Quite There Yet (
Xin et al. 2015), Psychiatry is the missing P in chronic pain care (
Howe & Sullivan, 2014), and my
previous post.
2 These tests measure “depression-like” and “anxiety-like” behaviors, respectively. We could certainly debate whether these are adequate models of depression and anxiety, and this was in fact the topic of an interesting discussion on
Twitter. The problem of anthromorphism is greatly magnified with concepts like the “
psychic pain” of separation distress (the
PANIC system of Panksepp and colleagues). For now, I'll refer you to my old post,
Of Mice and Women: Animal Models of Desire, Dread, and Despair.
3The world of dynorphin and KORs has gotten even more complicated since the discovery that subpopulations of dynorphin neurons in the nucleus accumbens have
opposing effects (aversion vs. reward). Crowley and Kash (2015) suggest that translation to humans may be..... uh difficult, to say the least:
“Important studies using modern genetic approaches have highlighted the multiple ways that KORs effect behavior, and paradoxical effects have emerged when manipulating the dynorphin system.”
...and...
“In addition, circuit and site-specific manipulations...provide some clarity as to the convoluted effect seen with systemic administration of KOR agonists. This provides key important information as to how KOR modulation can be used to shift anxiety-related behaviors: both low doses of KOR agonists, as well as KOR antagonists, may prove to be effective.”
...finally...
“Despite of an abundance of literature showing KORs to be a promising therapeutic target for the treatment of drug addiction ... few drugs impacting the KOR system have been taken to the level of human clinical trials.”
4 I haven't heard that morphine or buprenorphine is recommended for human babies who cry persistently and excessively.
5 @debe: in addiction it's 2 to 32 mg (pure bup) or to 24 (bup+nalox). 0.2 mg cps are for pain.
6The clinical trial was conducted in Israel, where buprenorphine is used to treat opioid dependence (as in many other countries) Litigiousness might be one possible reason such a study hasn't been conducted in the US?
7Caution is needed when interpreting results using
Last Observation Carried Forward (LOCF) analyses
– filling in missing values based on existing data
– because of the problematic nature of this method for handling missing data. See
Appendix below.
ReferencesCrowley NA, Kash TL. (2015).
Kappa opioid receptor signaling in the brain: Circuitry and implications for treatment.
Prog Neuropsychopharmacol Biol Psychiatry 62:51-60.
Howe CQ, Sullivan MD. (2014).
The missing 'P' in pain management: how the current opioid epidemic highlights the need for psychiatric services in chronic pain care.
Gen Hosp Psychiatry 36(1):99-104.
Kolodny A, Courtwright DT, Hwang CS, Kreiner P, Eadie JL, Clark TW, Alexander GC. (2015).
The prescription opioid and heroin crisis: a public health approach to anepidemic of addiction.
Annu Rev Public Health 36:559-74.
Panksepp, J., & Yovell, Y. (2014). Preclinical Modeling of Primal Emotional Affects (SEEKING, PANIC and PLAY): Gateways to the Development of New Treatments for Depression. Psychopathology, 47 (6), 383-393. DOI: 10.1159/000366208Tenore, P. (2008). Psychotherapeutic Benefits of Opioid Agonist Therapy. Journal of Addictive Diseases, 27 (3), 49-65. DOI: 10.1080/10550880802122646Watt, D., & Panksepp, J. (2009). Depression: An Evolutionarily Conserved Mechanism to Terminate Separation Distress? A Review of Aminergic, Peptidergic, and Neural Network Perspectives Neuropsychoanalysis, 11 (1), 7-51 DOI: 10.1080/15294145.2009.10773593Yovell, Y., Bar, G., Mashiah, M., Baruch, Y., Briskman, I., Asherov, J., Lotan, A., Rigbi, A., & Panksepp, J. (2015). Ultra-Low-Dose Buprenorphine as a Time-Limited Treatment for Severe Suicidal Ideation: A Randomized Controlled Trial. American Journal of Psychiatry DOI: 10.1176/appi.ajp.2015.15040535Yin X, Guven N, Dietis N. (2015).
Opioids in Depression: Not Quite There Yet.
UK Journal of Pharmaceutical and Biosciences 3(1):12-7.
AppendixReasons to avoid Last Observation Carried Forward (LOCF):
Streiner 2014: “...LOCF has serious and, in some cases, fatal problems.”
Olsen et al. 2012: “Although these methods are simple to implement, they are deeply flawed in that they may introduce bias and underestimate uncertainty, leading to erroneous conclusions.”
www.missingdata.org.uk: “For full longitudinal data analyses this is
clearly disastrous: means and covariance structure are seriously distorted. For single time point analyses the means are still likely to be distorted, measures of precision are wrong and hence inferences are wrong. Note this is true even if the mechanism that causes the data to be missing is completely random.”
Molnar et al. 2008:
“If there were a prize for the most inappropriate analytical technique in dementia research, 'last observation carried forward' would be the runaway winner.”Molnar et al. 2009: “The published results of some randomized controlled trials of dementia drugs may be inaccurate (i.e., drug effectiveness may be exaggerated) or invalid (i.e., there may be false-positive results) because of bias introduced through the inappropriate use of LOCF analyses.”